
By Veronica Amodeo
Patient-Centric Design
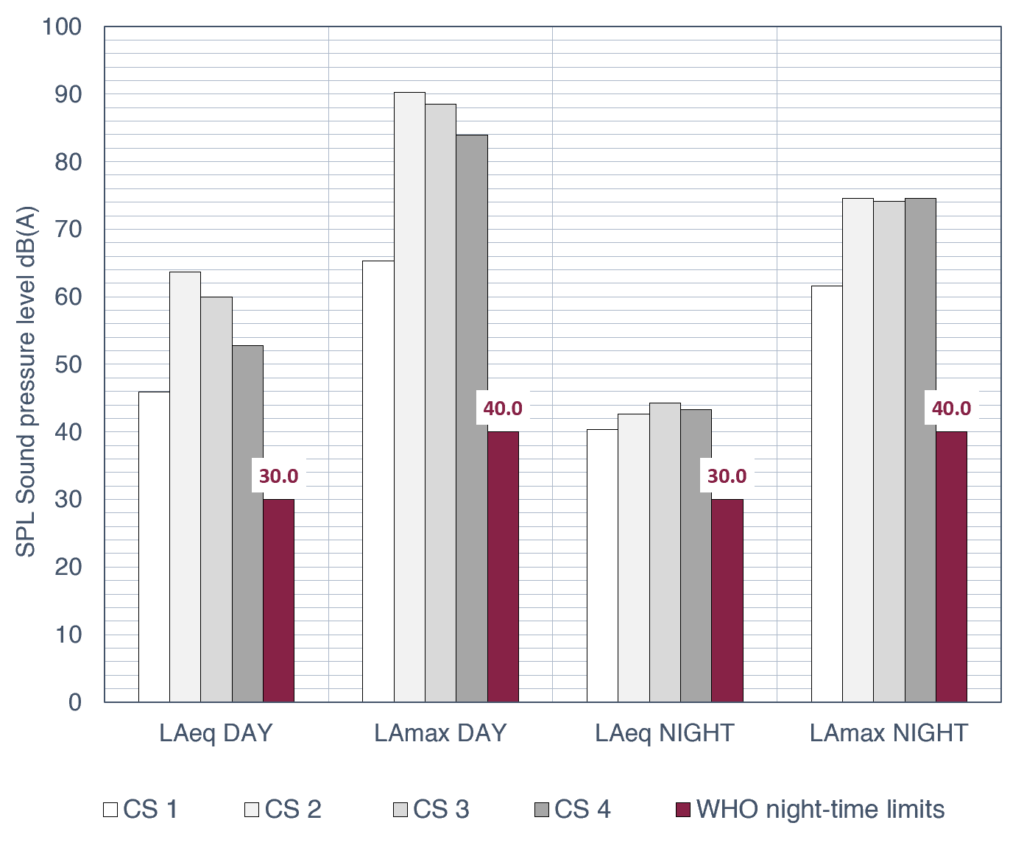
Hospital environments have a significant influence on patient recovery, not only through clinical care but also through environmental factors that impact biological, psychological, and social well-being. Among these factors, noise remains one of the most critical and yet insufficiently controlled stressors. Excessive sound exposure in healthcare settings has been linked to sleep disturbance, increased stress, impaired communication, and delayed recovery. The World Health Organisation recommends that sound pressure levels in patient areas should not exceed 30 dBA (LAeq) throughout the day and night, with peak levels maintained below 40 dBA (LAmax) to prevent disturbance. Despite these guidelines, international studies consistently report sound levels in hospitals that exceed recommended limits, highlighting the need for a deeper understanding of the impact of noise.
Evaluating the acoustic quality of a hospital environment, we must consider not only the sound pressure levels but also several qualitative dimensions:
- Types of sources: the specific types of sources that generate the local soundscape.
- User sensitivity: The subjective perception and vulnerability of those inhabiting these spaces, including both patients and healthcare staff, with different kinds of needs.
- Sound propagation: How noise travels through the ward, which is determined by the architectural layout and the performance of building elements. As architects, we have the opportunity to study how sound propagates within the inpatient area and, consequently, design acoustically efficient spaces.
1. Sound pressure levels and types of sources
To understand the acoustic context of the ward, we conducted SPL and spectra monitoring and structured observations across four hospital wards. The results consistently showed sound levels that far exceeded the WHO recommendations (Figure 1).
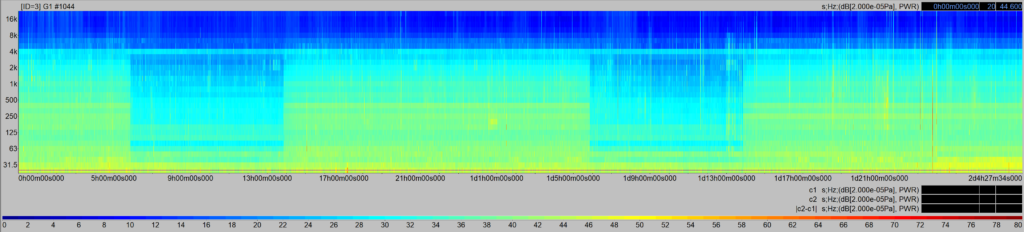
However, the data revealed that absolute decibel levels alone fail to capture the complexity of the hospital soundscape. Within the ward, the sound fluctuates constantly, creating a complex layering of continuous, intermittent, and impulsive sources with unique spectral profiles (Figure 2).
In our last preliminary work, we analysed everyday hospital sounds—such as stretchers, alarms, and speech— by applying Zwicker’s psychoacoustic model and the parameter of intrusiveness (UNI/TS 11844:2022 standard). Sounds like a passing stretcher or a ward phone can reach “Medium” to “High” intrusiveness levels because they emerge prominently from the background noise, regardless of their absolute LAeq. Intrusiveness was found to be well-correlated with loudness. Conversely, annoyance is significantly influenced by temporal and spectral characteristics, such as sharpness, fluctuation strength, and roughness. While the intrusiveness of a source provides additional information beyond global sound pressure levels, analysing spectral characteristics allows for a deeper understanding of the acoustic phenomenon [1].
2. Sound Propagation and Ward Organisation
The internal organisation of the ward has evolved over time to become the highly functional space we see today, designed to prioritise both patient safety and care efficiency. This layout ensures proximity between healthcare staff and patients for rapid assistance. Consequently, it is common to find open-plan workstations and staff-dedicated rooms located immediately adjacent to patient rooms. Combined with the widespread clinical practice of keeping bedroom doors open for constant visual and auditory control, the corridor becomes more than just a transit area. It acts as a primary hub for care activities where sound consequently propagates directly into the adjacent patient rooms.
3. The “Open-Door” Challenge in Patient Rooms
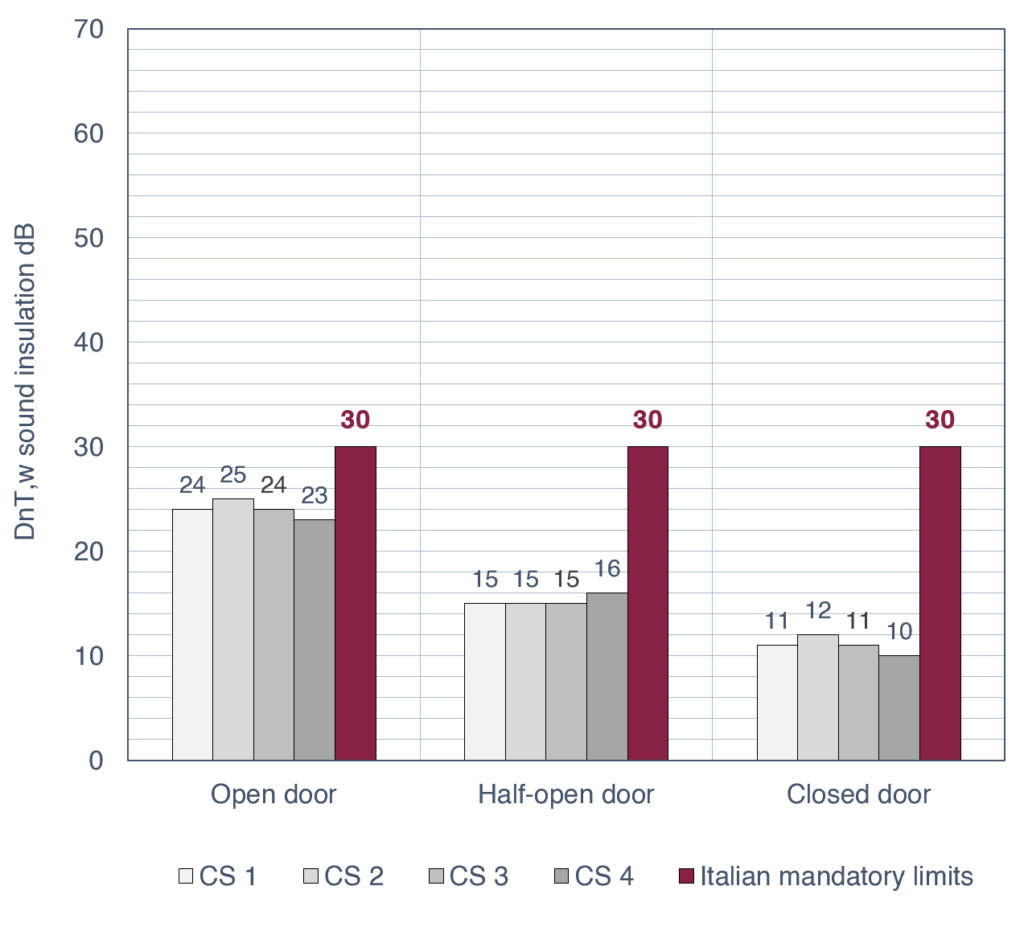
Since doors must stay open for safety, the traditional acoustic barrier effectively disappears. During my PhD program, we measured the normalised sound insulation (DnT,w) of the walls between the corridor and bedrooms in four case studies, using three door conditions: closed, half-open, and fully open.
While Italian standards require DnT,w = 30 dB, a typical room in our study dropped from an average of 24 dB (closed) to 15 (half-open) to 11 dB when fully open (Figure 3).
However, this 11 dB value represents the “residual” insulation provided primarily by the geometry of the room’s entrance and the materials of its surfaces, independent of the door’s performance. This finding suggests that probably the entrance zone—regardless of whether the door is kept open or closed—can be intentionally designed to act as an “acoustic filter”.
4. Acoustic strategy simulation
Our research goal was to enhance the humanisation of care by providing a quiet space without compromising the staff’s ability to monitor the patient.
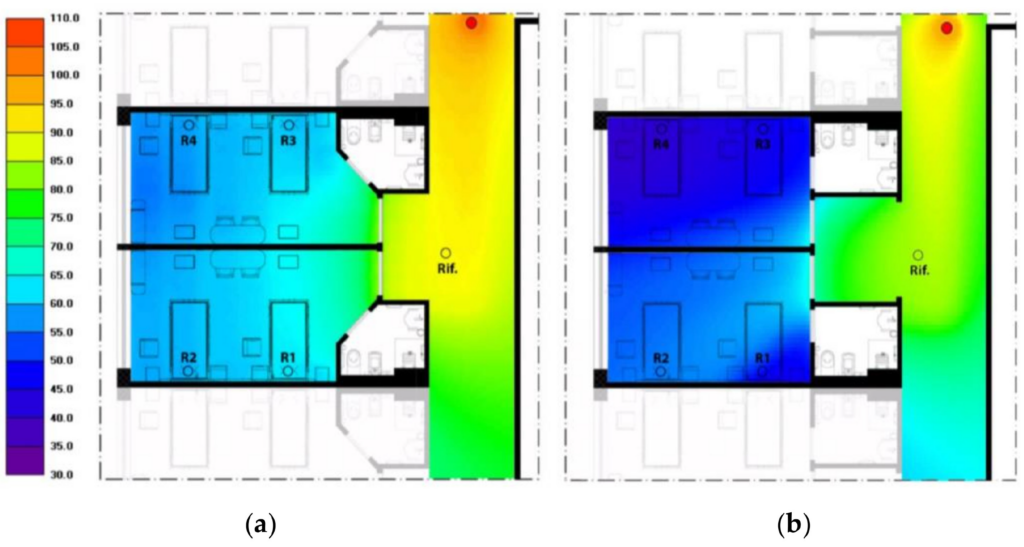
Therefore, in Case Study 1, we simulated a new access space using ray-tracing software. While maintaining the original partitions, we introduced two strategic changes: first, a different entrance shape; second, an application of sound-absorbing panels to the walls and to the ceiling (cavity mount) of the alcove. The goal was to ensure that sound waves coming from the corridor would reflect off these surfaces before reaching the patient’s bed, thereby losing energy through reflections on the sound-absorbing treatment [2].
The simulation confirmed that the “acoustic filter” achieved an additional sound pressure level reduction of approximately 11 dB at the patient’s bedside, even with the door fully open. A reduction of more than 10 dB is perceived by the human ear as a significant decrease in loudness. By effectively “halving” the perceived noise, we can significantly mitigate the intrusiveness of ward activities, thereby protecting the patient’s sleep and psychological well-being (Figure 4).
5. Conclusions: Patient-Centric Design
Given these findings, as the corridor represents the primary source of potentially disruptive noise, the architectural design must minimise reverberation times and reflections both within the corridor and at the room’s threshold. By strategically implementing sound-absorbing materials and optimised geometries, we can achieve a predictable and measurable reduction in the noise levels that ultimately reach the patient’s bed.
The future challenge for healthcare architecture will be to fully integrate psychoacoustic evidence—addressing not just the sound levels, but the temporal and spectral ‘texture’ of hospital sounds—into the design and organisational process. This shift marks a transition toward a context-driven acoustic design, where spaces are engineered to respond specifically to the unique environment of the hospital.
[1] D. De Salvio, V. Amodeo, M. Garai, S. Secchi, Noise assessment within healthcare facilities, Forum Acusticum 2025 Malaga (SP).
[2] S. Secchi, N. Setola, L. Marzi, V. Amodeo, Analysis of the acoustic comfort in hospital: the case study of Maternity rooms, Buildings, 2022, 12(8),1117; DOI: 10.3390/buildings12081117
……………………………………………………………………………………………………………………………………………………………………………………………………………………………………
For more information on this study, please reach out to Veronica Amodeo, Arch. PhD