
At the International Congress on Sound and Vibration (ICSV32) in Istanbul, several presentations highlighted a topic that is becoming increasingly difficult to ignore: the sound environment in healthcare facilities. While healthcare has made enormous advances in patient safety, technology and clinical outcomes, the acoustic environment often remains overlooked. Two presentations in particular caught my attention because they approached the issue from different angles—one through objective acoustic measurements and the other through the experiences of hospital users. Together, they reinforce a clear message: improving the hospital soundscape should be a priority in design and operation.
ICU Noise Levels: A Global Problem Exposed by Long-Term Measurements
In his presentation “Assessments of Acoustic Environments in Critical Care Units Across Multiple Countries,” Professor Pyoung-Jik Lee presented one of the most comprehensive international studies of intensive care unit (ICU) acoustics conducted to date.
The study was motivated by a challenge familiar to many researchers in hospital soundscape: previous studies have reported widely varying noise levels, often using different measurement methods, equipment and measurement durations. Some measurements have even been conducted with uncalibrated devices, making comparisons difficult.
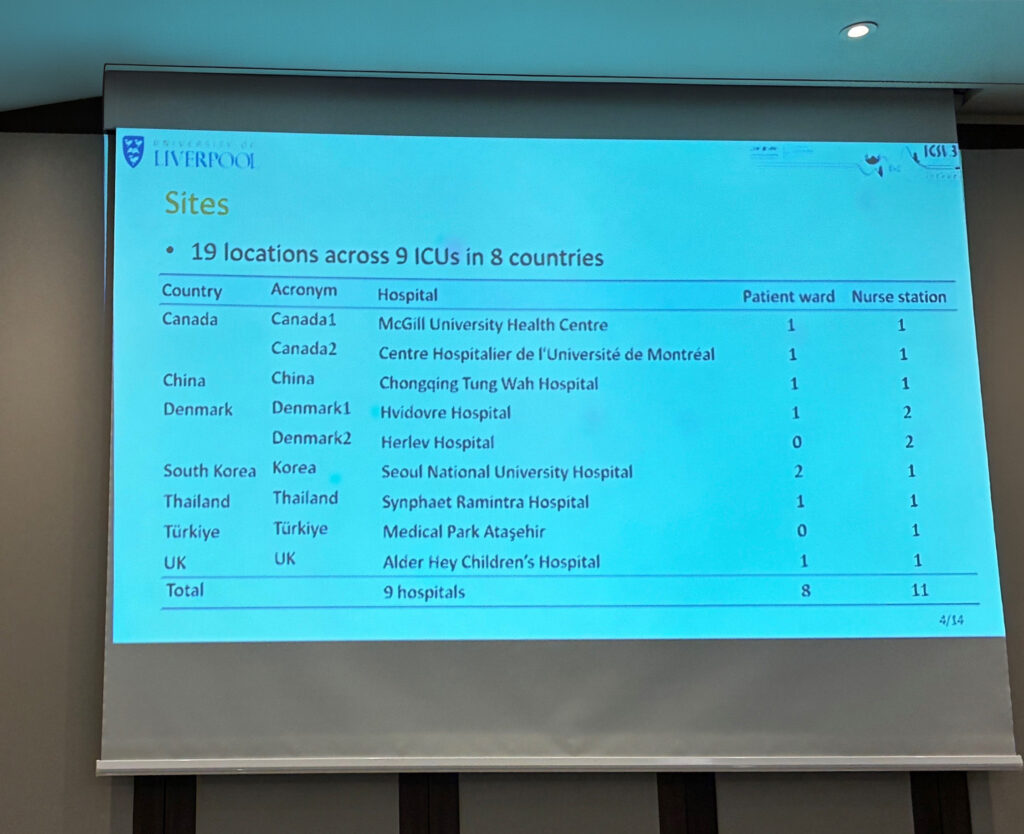
To address this, the research team established a standardised measurement protocol across nine hospitals in eight countries. Class 1 sound level meters were installed in patient areas and nursing stations, collecting data continuously for approximately two weeks.
The results were striking.
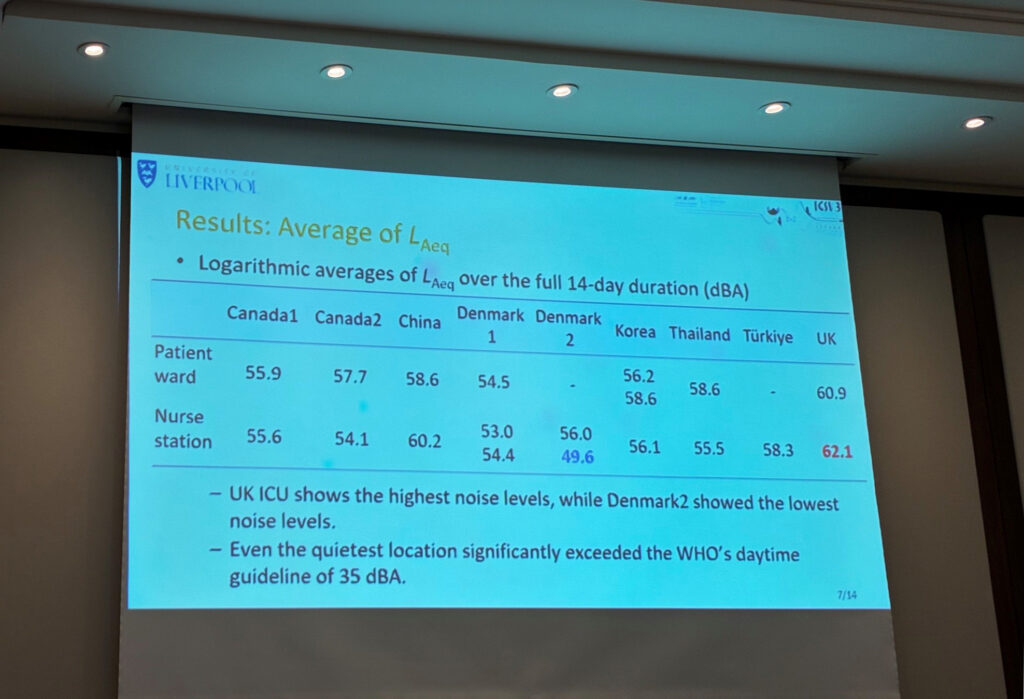
All ICU sites exceeded the World Health Organization’s recommended hospital noise level of 35 dB(A)*. Average sound levels ranged from approximately 50 dB(A) to over 62 dB(A), depending on the location. Even the quietest ICU was substantially above recommended limits.
The study also demonstrated substantial variation between hospitals, countries and even individual wards. Some locations showed relatively stable sound levels over time, while others fluctuated significantly from day to day. This finding highlights an important methodological lesson: short-term measurements may not accurately represent the true acoustic conditions of an ICU. A single day of measurement could either underestimate or overestimate the actual sound environment.
Another important finding concerned high-level noise events. While average sound levels were already elevated, maximum noise levels and the frequency of loud events were even more concerning. Some sites experienced a large proportion of sounds exceeding 60–70 dB(A), levels known to be disruptive for sleep, communication and recovery.
The researchers pointed to several contributing factors in hospital soundscape, including ward layout, clinical activities and building design. One example from a new UK hospital revealed surprisingly high background noise levels from building services alone. Even before patients, staff, and medical equipment were present, measured levels in patient rooms and corridors were already elevated.
For anyone involved in healthcare design, the implications are clear. Noise is not simply a consequence of hospital activity; it is also influenced by architectural and engineering decisions. The study provides valuable baseline evidence for future guidelines, noise mitigation initiatives and policies aimed at protecting both patients and healthcare workers.
Understanding the Hospital Through the Ears of Its Users
While Professor Lee’s research focused on measured sound levels, Samiha Yilmazer’s presentation “Exploring the Qualitative State Description Vector in the Oncology Clinic” explored how people actually experience the hospital environment.
The study was conducted in an oncology clinic and combined acoustic measurements with interviews and surveys involving patients, patient attendants and healthcare staff. The researchers argued that objective acoustic data alone cannot fully explain user satisfaction. Understanding how people perceive and interpret their environment is equally important.
The team conducted 30 semi-structured interviews and explored questions such as “What do people hear?” What would they like to hear? How do they feel in the environment?
Although the clinic exhibited different acoustic characteristics across the reception, waiting, and corridor areas, the measurements confirmed that sound levels exceeded the recommended maximum values throughout the facility. Yet an interesting observation emerged: many users had normalised the noise and viewed it as an unavoidable part of the hospital experience.
Patients and their attendants described the environment as noisy, dominated by conversations, machine sounds and background humming. However, acoustics were rarely their primary concern. Their experience was strongly shaped by waiting times, uncertainty and service expectations. As waiting times increased, participants became more negative in their assessment of the environment. Many sought quieter refuges or used headphones to cope, while still needing to hear when their name was called.
Healthcare staff viewed the same environment differently. Because they spend much longer periods in the space, they developed a greater awareness of its physical characteristics. Staff accepted some sounds as necessary but repeatedly highlighted the need for better sound insulation, greater privacy and quieter working conditions. They associated the environment with mental fatigue, headaches and difficulties maintaining privacy in open-plan settings.
One particularly interesting contribution from this study was the introduction of time spent in the environment as an important dimension in healthcare soundscape research. Patients, attendants and staff occupy the same physical space but experience it very differently because of the amount of time they spend there and the purpose of their visit. The researchers concluded that user type and duration of exposure strongly influence how hospital environments are perceived and evaluated.
A Common Message
Although these two studies used very different methods, they converge on the same conclusion.
The physical hospital soundscape frequently exceeds recommended levels, affecting both patients and staff. Objective measurements reveal the scale of the problem, while user-centred research helps us understand how noise is experienced in daily hospital life.
For those of us working with healthcare acoustics, this is encouraging. The growing body of evidence demonstrates that acoustics should not be treated as a secondary design consideration. Whether the goal is to support patient recovery, reduce staff fatigue, improve communication, or enhance privacy, sound matters.
The presentations at ICSV32 provided yet another reminder that creating healthier healthcare environments requires attention not only to what we can measure, but also to what people hear, experience and endure every day.
More reading on this topic:
Assessment of factors affecting speech in the ICU wards
* World Health Organization (1999) Guidelines for Community Noise. Geneva: World Health Organization.