
National standards in the Healthcare are lacking
In many countries, national standards, regulations, and guidelines in the healthcare sector are lacking and rarely include vertical absorption. One could therefore say that in many cases, building hospitals, elderly care homes, and psychiatric wards is the ‘wild west’ regarding acoustics. We are lucky when new buildings are built, because if there is a standard, we can follow it. The demands are often communicated in terms of reverberation time. The old buildings, on the other hand, are rarely suited to today’s purposes and activities. Reverberation time is a good indicator of a room’s acoustics, but it is challenging when it is the only descriptor.
A hospital has a complex task to solve, and the ‘old thoughts’ about reverberation time and acoustic material on a single surface as the only way to evaluate the room are not enough.
But what will it mean to the end users if we aim to evaluate other descriptors than reverberation time by implementing the thought of ‘vertical acoustics’? What happens when we realise that acoustic material on one surface only is so last decade?
A research study in Denmark
At Hvidovre Hospital in Denmark, a study took place a few years ago. The research aimed to determine the consequences of acoustic treatment for staff members. The scope was to find out whether vertical acoustics and better C50/D50 values would have any ‘extra’ effect on behaviour and attitude. Three identical rooms for an identical purpose (OR) were treated differently. Either no treatment, with an absorbing ceiling only or an absorbing ceiling and wall treatment. The study was designed as a blind study.
The results showed a clear tendency. In the room with both an acoustic ceiling (Class A) and wall panels, the staff felt less stressed and tired, and reported making fewer mistakes. It was predicted that the room with no treatment at all would be the least preferred. But the findings on the need for vertical acoustics were new and interesting.
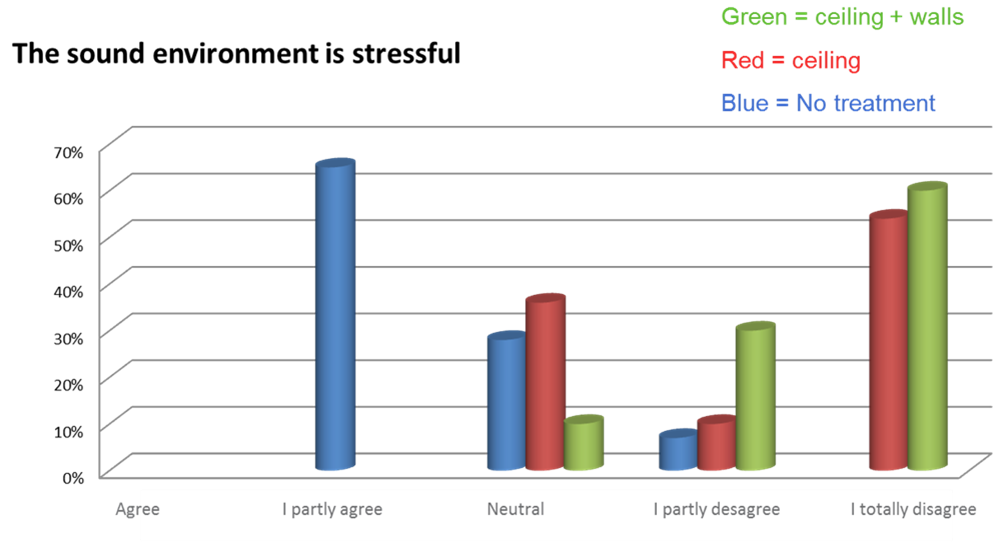
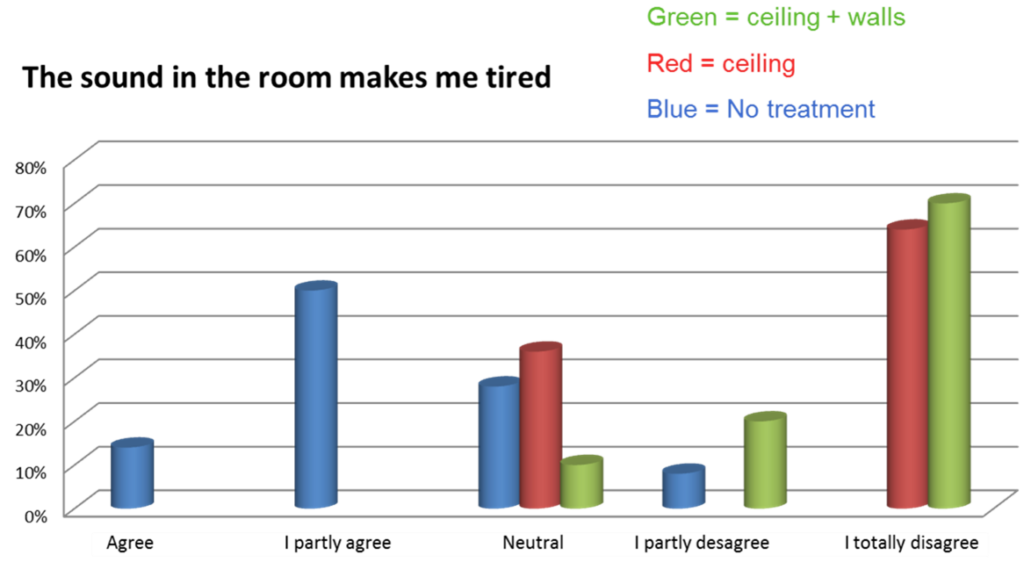
We need more research to understand what is important to both staff members and patients in healthcare facilities. This study really shows that evaluating more descriptors than reverberation time can be valuable. The numbers for reverberation time didn’t change much between the rooms with ceiling-only and ceiling-and-wall panels. However, D50 improved by almost 25%! The staff’s subjective response in this case may explain more than the obvious objective improvement in room acoustics. Read an interview with staff members from another hospital here.

Sabine and the diffuse sound field
The well-known Sabine equation is based on a theoretical condition that is unattainable in practice. A diffuse sound field. The typical acoustic solution in healthcare facilities uses absorption material on only one surface (the ceiling). And, according to the theory, the decay typically doesn’t follow a straight line. It will be split into an early part roughly corresponding to the theory. And a late part with a longer reverberation time. Furthermore, the grazing soundfield will not be evaluated using the formula.
Reverberation time is commonly measured over a 20- or 30-dB range. Starting 5 dB below the initial level, and then extrapolated to the full 60 dB range. Starting 5 dB below can be problematic since this part of the decay contains a lot of information. It contains both direct sound and early reflections, both of which are crucial for sound perception and speech clarity.
In other segments, research about other acoustic descriptors is developing. And the ISO3382-3 is a good example of how the understanding of activity-based design should look when we design offices. In Scandinavia, we also often see the Speech Transmission Index, Clarity C50, and/or Definition D50 used to evaluate classrooms. With the purpose to secure optimal room acoustics for the activity.
Within activity-based design, regardless of room type, reverberation time should not be the only descriptor.
Further reading on wall absorption: